

Smith A, Coles S, Johnson S, Saldana L, Ihekweazu. An outbreak of influenza A(H1N1)v in a boarding school in South East England, May-June 2009. Euro Surveill. 2009;14(27):pii=19263
Background
The first case of influenza A(H1N1)v in the United Kingdom (UK) was reported by the Health Protection Agency (HPA) on 27 April 2009 [1]. Following this initial report, the number of confirmed cases has risen steadily.
On 27 May 2009, a case of influenza A(H1N1)v was confirmed in a 14 year-old pupil at a boarding school in South East England. The case did not meet the HPA’s algorithm for testing at the time. The algorithm for testing of influenza A(H1N1)v at the time included travel to the United States or Mexico or contact with a probable or confirmed case. While this patient had influenza-like symptoms, there was no history of travel to an affected area or relevant contact. Swabs were taken from this pupil under the auspices of a private medical care service for independent schools. It subsequently became obvious that a significant outbreak was in progress in the school.
This paper describes the epidemiology and public health response to this outbreak. This is the first published report of an outbreak of influenza A(H1N1)v in a boarding school.
The index case and initial investigation
The index case became symptomatic on 24 May 2009, swabs were taken on 26 May and a positive result by PCR with primers specific for influenza A(H1N1)v [2] was received on 27 May. The positive result was notified to the local Health Protection Unit (HPU) on the evening of the same day, 27 May. The school was scheduled to close on the next day, 28 May, for a planned break during term time.
The initial risk assessment suggested that the index case had very limited contact with other pupils while symptomatic. His close contacts were identified as 15 other pupils who were also boarders at the school. All 15 close contacts were assessed for influenza-like illness (ILI), and offered post-exposure prophylaxis with oseltamivir, in accordance with HPA guidance at the time.
Following the identification of the first positive case, further enquiries were undertaken at the school by the HPA. It became apparent that there had been an ongoing outbreak of ILI at the school which preceded the confirmed diagnosis of influenza A(H1N1)v in the index case. A total of 39 cases had reported to the school’s health services with ILI prior to the identification of the index case on 27 May 2009. Following this finding, a decision was taken to extend the response beyond the initial 15 cases, to include the entire school population. Active case finding was initiated by asking all students and staff with ILI to telephone one of the nine “flu response centres” around the country for assessment. If appropriate, they were recommended testing and treatment. This was necessary as staff and students were dispersed across the country following the closure of the school for a short break. This led to the identification of further possible and probable cases associated with the school.
The HPA case definition was used: A possible case was any person meeting the clinical and epidemiological criteria; a probable case was any person meeting the clinical and epidemiological criteria and with a positive test for influenza A infection that was untypable at the local laboratories.
Descriptive epidemiology
Setting
The outbreak occurred in a boarding school in South East England with a total population of 2,132 made up of 1,307 pupils and 825 members of staff.
Case definition
Since it was obvious that there was a rise in the number of ILI cases before the index case, we considered these as “clinical” cases and included them in our description of the outbreak. We therefore categorised our cases into confirmed cases and clinical cases.
Confirmed cases were cases of influenza A(H1N1)v confirmed by laboratory testing of swabs taken while the patient is symptomatic with ILI.
Clinical cases were among pupils documented as attending a healthcare facility at the school with ILI from 1 May 2009 to the confirmation of the first case on 27 May 2009.
Outbreak description
In total, there were 102 symptomatic cases with ILI. Nose and throat swabs were taken from all cases symptomatic at the time the outbreak was detected. Influenza A(H1N1)v infection was laboratory-confirmed by PCR with primers specific for influenza A(H1N1)v in 63 of the 102 cases, 62 pupils and one member of staff. The remaining 39 cases were no longer symptomatic at the time the outbreak was recognised, and it was too late to take throat swabs. These 39 were classified as cases of ILI, epidemiologically linked in time and space to the confirmed cases.
The onset of the outbreak was estimated to have been on 1 May 2009 and the end on 3 June 2009. The school was closed from 28 May to 7 June 2009, extending the scheduled break by four days. The incubation period for influenza A(H1N1)v is unknown but estimated to be between one and seven days [3], therefore cases presenting with symptoms after 3 June 2009 were considered to have resulted from secondary transmission outside the school setting.
Potential source of exposure
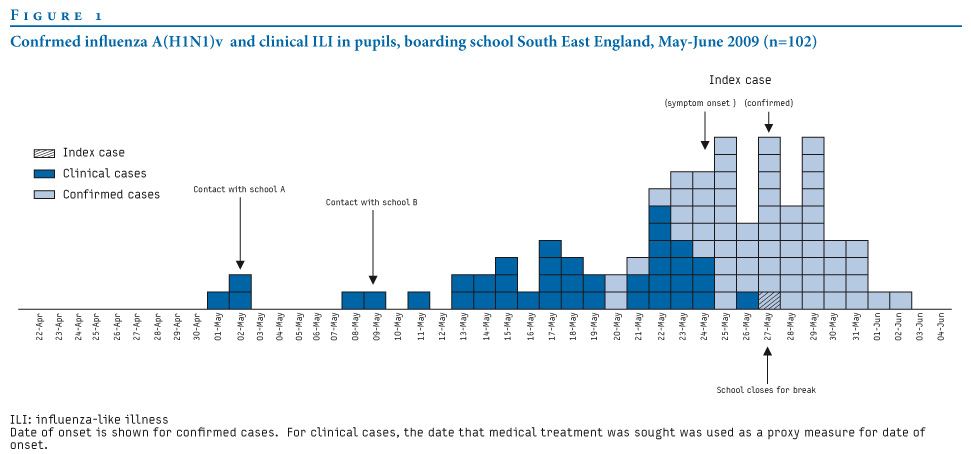
There were two potential points of contact between pupils from this boarding school and other schools (schools A and B in Figure 1) that had already had confirmed cases of influenza A(H1N1)v. No confirmed cases of influenza A(H1N1)v or clinical ILI cases were seen in the specific students who reported contact with students from school A during a social function. The second point of contact was with a group of students who visited school B for a tennis match on May 9. One of the students in contact with school B developed symptoms on 24 May 2009 and tested positive for influenza A(H1N1)v. Contact during this event may represent the source of the outbreak assuming that the ILI cases that occurred before this event may not have been due to influenza A(H1N1)v. School B had been closed due to an outbreak of influenza A(H1N1)v between 11 and 18 May 2009 in six members of staff and students.
The first confirmed case of influenza A(H1N1)v at the boarding school developed symptoms on 20 May 2009, pre-dating the onset of symptoms in the index case (27 May) by seven days (Figure 1). The incubation period for influenza A(H1N1)v is estimated to be between one and seven days indicating that there may have been ongoing transmission in the school from as early as 13 May 2009.
Figure 1. Confirmed influenza A(H1N1)v and clinical ILI in pupils, boarding school South East England, May-June 2009 (n=102)
Attack rates by house of residence and school year group
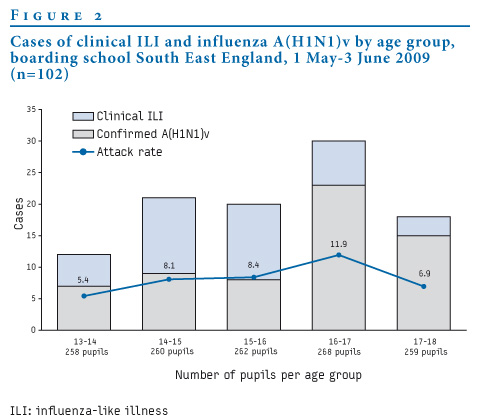
All school years and all houses of residence were affected by the outbreak. Taking the entire school population (pupils and staff), there was a clinical attack rate of 5% (102/2,132). However, given that the living circumstances of the students were significantly distinct from those of members of staff, the student population was considered as the affected cohort. Among the students, the clinical attack rate was 8% (101/1,307). The attack rates among the pupils were also calculated by house of residence as well as by school year (Figure 2). These attack rates varied by house, ranging from 1.8% (1/55) to 18.9% (10/53), as well as by school year, ranging from 5.4% (14/258) to 11.9% (32/268). The school year with pupils aged between 16 and 17 years had the highest attack rate of 11.9%.
Figure 2. Cases of clinical ILI and influenza A(H1N1)v by age group, boarding school South East England, with onset date 1 May - 3 June 2009 (n=102)
Clinical epidemiology
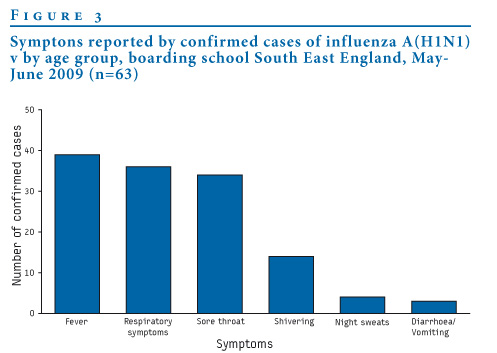
The distribution of symptoms among the cases is illustrated in Figure 3. These were typical of influenza-like illnesses. There were no hospitalised cases. Information on the duration of symptoms was not available.
Figure 3. Symptoms reported by confirmed cases of influenza A(H1N1)v, boarding school South East England, May-June 2009 (n=63)
The public health response
School closure
The school closed to all pupils from 27 May until 7 June 2009. The advice to close for seven days according to HPA guidance at the time became redundant as the school was already closed for a scheduled break for four days, and this break was extended by a further seven days as the school preferred to open on a Sunday. Those without symptoms of ILI who had their state exams scheduled for Monday, 1 June 2009, were permitted to return on 31 May, while the rest of the school remained closed. These pupils were assessed for symptoms, and if symptomatic, were offered anti-viral medicines and testing. They were permitted to take their exams under special conditions to minimise the risk of transmission.
Antiviral prophylaxis
Following the identification of additional probable and possible cases associated with the school, the HPA’s advice of prophylaxis was extended beyond the initial group of close contacts to all staff (n=825) and students (n=1,307) attending the affected school. Despite the HPA’s advice, the estimated uptake of antiviral prophylaxis among those for whom it was recommended was only 48%. We do not know whether cases occurred in those who took the oseltamivir and do not have information on why the uptake of prophylaxis was not higher. These issues will be explored in a subsequent study.
Information to parents
Parents were informed by letter that the school had a confirmed case of influenza A(H1N1)v and that the school would close until 7 June 2009. A second letter was subsequently issued detailing advice to offer antiviral prophylaxis to all the pupils and staff at the school.
Clinic at school
An assessment and collection point was established at the college to offer assessment and treatment to returning students, staff members and families of resident staff.
Discussion and conclusion
This outbreak represents the first in a boarding school. The index case had no associated travel history or clear contact with a confirmed or probable case. The other school outbreak described in the literature [4] , in New York, United States, involved 45 confirmed cases.
The initial risk assessment following the identification of the index case indicated there were few close contacts, and therefore post-exposure prophylaxis was limited to this group. It became evident during the investigation that the school had had an ongoing outbreak of ILI in the weeks prior to the identification of the index case. It is likely that many of these cases of ILI were due to influenza A(H1N1)v. Swabs taken from some of these cases who were still symptomatic identified a further three confirmed cases. Influenza A(H1N1)v could not be confirmed in most of the earlier cases of ILI as they were no longer symptomatic at the time the outbreak was detected. The source of the outbreak in this school was probably contact with pupils in another school with confirmed cases. This outbreak will add evidence to the hypothesis that the number of confirmed cases of influenza A(H1N1)v underestimates the burden of disease as has been reported previously [5].
It has been evident from previous reports (including unpublished data) that schools represent an important location for transmission [1]. The reported symptoms suggest an illness of no worse severity than seasonal influenza. None of the cases were hospitalised. While all school years and houses were affected, there was considerable variation in the attack rates between boarding houses. Further insight into this variation will depend largely on gaining some understanding of the transmission dynamics following the first case in the school and the extracurricular and social activities the pupils participated in while exposed to symptomatic cases.
Control measures were implemented as soon as the index case was confirmed. The school closed on 27 May 2009 and post-exposure prophylaxis was offered to the whole school from 31 May 2009. Had the outbreak had been detected earlier, the school closed earlier and prophylaxis commenced after the initial cases were detected according to the HPA’s guidance at the time, we may have seen lower levels of transmission within the school.
Acknowledgements
We will like to acknowledge the contribution of Gail Fairbairn for diligently supporting the data management for this report, and all our colleagues in the Flu Response Centres across England who rose to the challenge at very short to offer treatment and prophylaxis to the school population
References
- Health Protection Agency, Health Protection Scotland, National Public Health Service for Wales, HPA Northern Ireland Swine influenza investigation teams. Epidemiology of new influenza A (H1N1) virus infection, United Kingdom, April – June 2009. Euro Surveill. 2009;14(22):pii=19232. Available from: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19232
- Ellis J, Iturriza M, Allen R, Bermingham A, Brown K, Gray J, et al. Evaluation of four real-time PCR assays for detection of influenza A(H1N1)v viruses. Euro Surveill. 2009;14(22):pii=19230. Available from: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19230
- Centers for Disease Control and Prevention (CDC). Interim Guidance for Clinicians on Identifying and Caring for Patients with Swine-origin Influenza A (H1N1) Virus Infection. Atlanta: CDC; 2009 May 4. Available from: http://www.cdc.gov/h1n1flu/identifyingpatients.htm
- Centers for Disease Control and Prevention (CDC). Swine-origin influenza A (H1N1) virus infections in a school - New York City, April 2009. MMWR Morb Mortal Wkly Rep. 2009;58(17):470-2.
- Novel Swine-Origin Influenza A (H1N1) Virus Investigation Team, Dawood FS, Jain S, Finelli L, Shaw MW, Lindstrom S, et al. Emergence of a Novel Swine-Origin Influenza A (H1N1) Virus in Humans. N Engl J Med. 2009;360(25):2605-15.
See Also:
Latest articles in those days:
- Birth cohort effects in adults associated with influenza A(H1N1)pdm09 vaccine effectiveness 2 hours ago
- Genetic Characterization of Swine Influenza Viruses in Thailand in 2019-2025 Reveals Novel Reassortants 2 hours ago
- Outbreak dynamics of high pathogenicity avian influenza virus H5N1, clade 2.3.4.4b euBB, in black-headed gulls and common terns in Germany in 2023 3 hours ago
- [preprint]The canine respiratory epithelium is a permissive ecosystem for influenza interspecies transmission and emergence 3 hours ago
- [preprint]Explainable and Calibrated AI for Decoding Host-Adaptive Changes in Influenza A Virus 3 hours ago
[Go Top] [Close Window]